 The principal sponsor of the Vermont ACEs bill, Dr. George Till, has an ALE (not a typo) score of at least one. He describes losing six of seven sections of the ACEs legislation as an “Adverse Legislative Experience (ALE)”. But if re-elected this November, he plans to “push again next session” for provisions to embed the ACEs research findings into medical practice. While “extremely disappointed” with the outcome of the conference committee dropping most of his bill’s provisions, his resiliency is evident as he looks ahead to the next opportunity to improve health outcomes.
The principal sponsor of the Vermont ACEs bill, Dr. George Till, has an ALE (not a typo) score of at least one. He describes losing six of seven sections of the ACEs legislation as an “Adverse Legislative Experience (ALE)”. But if re-elected this November, he plans to “push again next session” for provisions to embed the ACEs research findings into medical practice. While “extremely disappointed” with the outcome of the conference committee dropping most of his bill’s provisions, his resiliency is evident as he looks ahead to the next opportunity to improve health outcomes.
On May 10, the last day of the Vermont legislature, a broad healthcare bill (H. 596) passed that included the one remaining ACEs provision. This section mandates a review by Jan. 15, 2015 of “evidence-based materials on the relationship between adverse childhood experiences (ACEs) and population health and recommend to the General Assembly whether, how, and at what expense ACE-informed medical practice should be integrated into
Blueprint practices and community health teams.” (The original legislation called for exploring ways to implement the “use of an appropriate and voluntary screening tool containing questions on the ten categories of the ACEs,” appropriate training for providers using a screening tool, and financial incentives to encourage the use of the tool. See the ACEsTooHigh post on the original legislation.)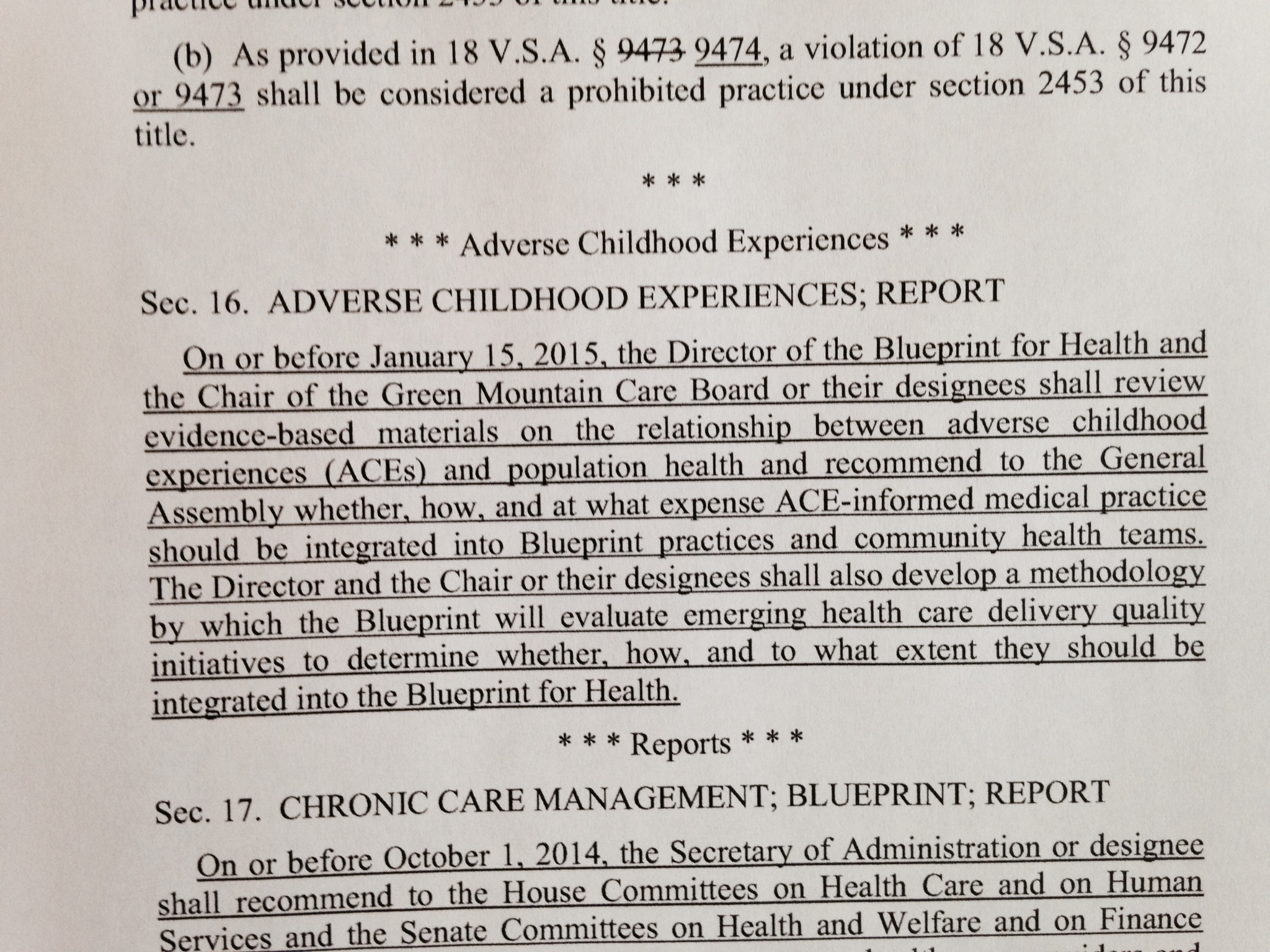
The review of evidenced-based materials in the new law is to be conducted by the director of the Blueprint for Health (a state-led health care program that includes the majority of Vermonters) and the chair of the Green Mountain Care Board (a body created by the legislature in 2011 to regulate health insurance rates and hospital budgets) or their designee.

The legislation also charges the director of the Blueprint and chair of Green Mountain Care Board with developing “a methodology by which the Blueprint will evaluate emerging healthcare delivery quality initiatives to determine whether, how and to what extent they should be integrated into the Blueprint for Health.” This evaluation of quality initiatives in tandem with the ACEs review could provide valuable new directions in health care system reform in Vermont, especially if the two processes inform one another. Value added is another provision dealing with chronic care management, specifically citing conditions such as obesity, mental conditions, and oral health.
Till has not decided what exact provisions he will advance in the next session, but among the ideas he is considering are “a pilot of parenting classes run out of OB/GYN offices,” and the inclusion of ACEs content in physician and medical student education.
Provisions related to ACEs educational content in the original legislation include:
- The University of Vermont College of Medicine and School of Nursing shall consider adding or expanding information to their curricula about the ACE Study and the impact of ACEs on lifelong health.
- Vermont Board of Medical Practice and the Vermont Medical Society Education and Research Foundation shall develop educational materials pertaining to the ACE Study, “including available resources and evidence-based interventions for physicians, physician assistants, and advance practice registered nurses.”
Another provision dropped from the bill required the Department of Health to report to the Green Mountain Care Board recommendations to incorporate education, treatment and prevention of ACEs into the state’s medical practices and the Department of Health, on the availability of appropriate screening tools and evidence-based interventions, and on additional security protections for patients.
Also left on the cutting room floor were pilot programs for counties and primary schools using the Vermont Family Based Approach (developed by the Vermont Center for Children, Youth, and Families to address children’s emotional-behavioral health, promote family health and treat behavioral problems using a family based approach) and the designation of a director of Adverse Childhood Experience, Treatment and Prevention within the Department of Health.
If Till is re-elected this November, he will have the opportunity to build on what he learned and craft a new ACEs bill for the 2015 session, and transform his ALE into a PLE (Positive Legislative Experience). While the Vermont ACEs legislation may be a baby step, it nevertheless makes Vermont the second state, after Washington State, to enact an ACEs statute. The process that unfolded in Washington, cumulating in the enactment of an ACEs law in 2011 (HB 1965), was more protracted and fraught than the one in Vermont. In the end, the law validated a nascent public-private partnership and declared the state’s commitment to investing in the positive development of children and preventing and mitigating the effects of adverse childhood experiences (ACEs). A subsequent post will provide more information on the Washington law and the ongoing work of the Washington State ACEs Public Private Initiative (APPI).

[…] session, Rep. George Till was picking himself up, dusting himself off and reflecting on what he called an “ALE…..or Adverse Legislative Experience” when his ambitious legislative vision fizzled into a tiny bubble of hope to create a […]
LikeLike
[…] this gave momentum to the state’s trauma-informed schools movement. Earlier this year, Vermont passed a limited but meaningful provision in a larger health bill to evaluate whether ACE-informed medical practice should be included in […]
LikeLike
[…] this gave momentum to the state’s trauma-informed schools movement. Earlier this year, Vermont passed a limited but meaningful provision in a larger health bill to evaluate whether ACE-informed medical practice should be included in […]
LikeLike
[…] resolutions also serve an invaluable educational purpose. As the prime sponsor for the Vermont ACEs bill, Dr. George Till, said that the “Whereas” section of his bill was a place to highlight the most compelling data […]
LikeLike
[…] resolutions also serve an invaluable educational purpose. As the prime sponsor for the Vermont ACEs bill, Dr. George Till, said that the “Whereas” section of his bill was a place to highlight the most compelling data […]
LikeLike
Yeah! Nice work! I can imagine how hard it can be to legislate care when so much is about money.
LikeLike